


 2527
2527
 Share
Share



Abstract
Background: Cow’s Milk Protein Allergy (CMPA) is one of the most prevalent food allergies in children and frequently turns into “allergic march”, progressing from food allergy to atopic dermatitis and subsequently to childhood asthma. Modern treatment primarily works on allergen avoidance and symptomatic relief without finding out the underlying immune-digestive dysfunction. Ayurveda correlates CMPA with Ksheer Alasaka resulting from Ahar Asatmya, Agnimandya, and Kapha-Pradhana Tridoshaja Dushti, leading to Vicharchika and Shwasa Roga.
Objective: To evaluate the effectiveness of Ayurvedic management in a pediatric patient suffering from cow milk allergy associated with atopic dermatitis and childhood asthma.
Materials and Methods: A 9-year-old female child diagnosed with cow milk allergy, with atopic dermatitis and recurrent childhood asthma, was treated at IAFA using a personalized Ayurvedic protocol. Management included formulations such as Total Care 3X Ras, Respiratory Care X Drops, Respiro Detox Formula, Aahar Amrutham Bindu, and Aahar Amrutham Ras, etc., along with dietary regulation and allergen avoidance. Total treatment duration was 5 months with regular follow-ups.
Results: Progressive reduction in respiratory attacks, complete resolution of skin itching and dryness, normalization of bowel habits, and sustained remission without recurrence were observed at 5-month follow-up.
Conclusion: Ayurvedic management based on Ahar Asatmya Chikitsa, Agnideepana, Kapha-Vata Shamana, Stroto Shodhana, and Rasayana principles successfully reversed cow milk allergy with allergic march, highlighting the gut-immune-skin-airway axis correction as a root therapeutic target.
Introduction
Cow’s Milk Protein Allergy (CMPA) is one of the most prevalent food allergies in infancy and early childhood and represents a major contributor to the development of chronic allergic diseases.[1] It is estimated that cow milk proteins, particularly α-S1-casein and β-lactoglobulin, are responsible for IgE-mediated and non-IgE-mediated immune reactions that manifest through the gastrointestinal, cutaneous, and respiratory systems.[2,3] CMPA frequently serves as the first step of the allergic march, a progressive pattern in which early food allergy is followed by atopic dermatitis and subsequently evolves into allergic rhinitis and childhood asthma.[4,5]
Clinically, CMPA may present with colicky abdominal pain, regurgitation, constipation or diarrhea, but in many children it extends beyond the gut to produce persistent eczema and wheezing disorders.[6] The association between food allergy, atopic dermatitis, and childhood asthma has been well documented in pediatric immunology literature, which describes shared immunopathological pathways involving Th2 polarization, elevated IgE levels, mast cell activation, and chronic mucosal inflammation. These mechanisms result in persistent epithelial barrier dysfunction of the gut and skin, allowing continued allergen penetration and immune hyperresponsiveness, thereby sustaining the allergic march.[7]
Modern treatment of CMPA primarily depends on strict elimination of cow milk and milk products, symptomatic treatment of eczema with topical corticosteroids or emollients, and bronchodilators or inhaled corticosteroids for asthma control.[8] Although this line of treatment reduces symptom severity, it does not correct the underlying immune-digestive dysregulation and often results in long-term dependency on pharmacotherapy with potential adverse effects. Consequently, a significant proportion of children continue to experience recurrent flares and progression of allergic disease despite compliance with dietary avoidance.
From the Ayurvedic perspective, food hypersensitivity is conceptualized under Ahar Asatmya, i.e., intolerance to specific food substances arising from Agnimandya, i.e., impaired digestive and metabolic capacity. Cow milk allergy is described in classical texts under the condition Ksheer Alasaka, in which the heavy, Kapha-Vardhaka properties of milk disturb the digestive fire, leading to accumulation of Ama, i.e., undigested toxic metabolites.
This Ama circulates systemically, vitiating Kapha predominantly and subsequently Vata and Pitta, resulting in obstruction of microchannels (Strotorodha). When this pathological process involves the skin, it manifests as Vicharchika, i.e., atopic dermatitis, and when it affects the respiratory system through Pranavaha Strotas Dushti, it produces Shwasa Roga, i.e., childhood asthma. Thus, Ayurveda considers CMPA not as an isolated disorder but as a systemic disease of digestion-immune dysfunction affecting multiple organ systems.
The present case report represents a 9-year-old female child suffering from cow milk allergy associated with atopic dermatitis and childhood asthma, demonstrating the classical progression of allergic march. The child was treated at the Institute of Applied Food Allergy (IAFA) using a phase-wise Ayurvedic protocol focused on correction of Ahar Asatmya, restoration of Agni, elimination of Ama, and normalization of Kapha-Vata imbalance, leading to sustained remission without recurrence.
Case Study
This case report describes a 9-year-old female child who presented to the Institute of Applied Food Allergy (IAFA) with long-standing complaints of cow milk allergy associated with progressive involvement of the skin and respiratory system, clinically representing the classical pattern of allergic march.
The child had been receiving only symptomatic treatment for atopic dermatitis and asthma for several years, without identification of the underlying food intolerance, resulting in recurrent exacerbations and repeated hospitalizations. A detailed Ayurvedic evaluation and food intolerance testing revealed cow milk protein allergy as the central etiological factor responsible for multisystem allergic manifestations.
1) Patient Details
Age / Gender – 9 years / Female
Date of Registration – 13 September 2020
Duration of Illness – Approximately 4 years
Past History – Recurrent childhood asthma requiring hospitalization, chronic itchy skin lesions
Family History – Not significant
2) Chief Complaints
Gastrointestinal:
- Colicky abdominal pain
- Regurgitation and nausea
- Chronic constipation with occasional perianal rash
Skin:
- Atopic dermatitis
- Severe itching, predominantly over the flexural areas of the feet
- Dry and rough skin
Respiratory:
- Recurrent rhinitis
- Chronic cough
- Wheezing and frequent asthmatic attacks requiring hospitalization
3) Diagnosis
Modern Diagnosis: Cow Milk Protein Allergy associated with Atopic Dermatitis and Childhood Asthma.
Ayurvedic Diagnosis:
- Ksheeralasaka
- Kapha-pradhana Tridoshaja Dushti
- Vicharchika with Swasa Roga
4) Common Triggering Allergens
Food and environmental allergens identified through food intolerance testing were:
Food Allergens:
- Cow milk
- Almond
- Curd
- Cheese
- MSG (Ajinomoto)
- Chana dal
- Orange
- Cocoa
- Rice
Environmental Allergens:
- House dust mite
- Dog Dander
Drug Sensitivity:
- Paracetamol
Materials And Methods
The child was managed at IAFA using a phase-wise Ayurvedic treatment protocol aimed at correcting food intolerance, restoring digestive-immune balance, and preventing recurrence of allergic manifestations. Baseline clinical assessment included detailed history, systemic examination, Ashtavidha Pariksha, and food intolerance testing to identify causative allergens. Treatment was individualized and modified according to clinical response at each follow-up.
1) Intervention Protocol
The therapeutic strategy was designed to:
- Correction of Ahar Asatmya and Agnimandya
- Elimination of Ama and pacification of Kapha
- Restoration of gut barrier integrity and immune tolerance
- Clearance of Pranavaha Strotas obstruction to stabilize respiration
- Prevention of allergic progression and recurrence
Parents were counseled regarding strict avoidance of identified food and environmental allergens throughout the treatment period.
2) Ayurvedic Treatment Protocol (First visit-September 2020)
| Formulation | Dose | Route | Therapeutic Action |
| Total Care 3X Ras | 10 ml BID | Oral | Anti-allergic, Kapha-Vata Shamana, bronchodilator |
| Respiratory Care X Drops | 10 drops BID with water | Oral | Strengthens the respiratory system, anti-asthmatic |
| Respiro Detox Formula | 2 g BID with honey | Oral | Clears airway obstruction, mast-cell stabilization |
| E-5 Cell Repair Oil | Local application | External | Relieves atopic dermatitis, skin healing |
| IAFA Skin Fresh Bar | Daily bath | External | Anti-inflammatory, reduces itching and dryness |
3) Phase-wise Ayurvedic Management During Follow-ups
| Phase | Duration | Formulations Prescribed | Therapeutic Goal |
| Phase I-Allergy Control and Respiratory Stabilization | Sept-Oct 2020 | Total Care 3X Ras, Respiratory Care X Drops, Respiro Detox Formula, E-5 Cell Repair Oil, Skin Fresh Bar | Reduce allergic reactivity, stabilize asthma, and initiate gut-immune correction. |
| Phase II-Consolidation Phase | Oct-Dec 2020 | Above medicines along with Haridra Khandam, Laxmi Vilas Ras | Control skin inflammation, prevent asthma recurrence |
| Phase III- Gut Repair and Immunomodulation | Jan-Mar 2021 | Aahar Amrutham Bindu, Aahar Amrutham Ras, Haridra Khandam, IAFA skin fresh bar | Restore gut integrity, improve immune tolerance, prevent relapse. |
4) Dietary Recommendations
- Complete avoidance of cow milk and all milk products.
- Elimination of identified allergens, including almonds, cheese, curd, cocoa, MSG, chana dal, orange, and rice.
- Warm, freshly prepared meals are advised.
- Avoidance of refrigerated, fermented, and junk foods.
- Avoidance of incompatible food combinations, such as milk with salty or non-vegetarian food.
- Focus on a light, easily digestible diet to maintain Agni and prevent Ama formation.
5) Monitoring Parameters
- Clinical response was monitored monthly based on:
- Frequency of asthma attacks and need for hospitalization
- Severity of skin itching and dermatitis lesions
- Gastrointestinal symptoms such as constipation and abdominal discomfort
- Requirement of any allopathic rescue medication
Results
The patient was followed for five months with regular monthly assessments. Clinical outcomes were evaluated on the basis of respiratory symptoms, dermatological manifestations, and gastrointestinal complaints. A symptom-severity scoring system was used (0 = absent, 1 = mild, 2 = moderate, 3 = marked, 4 = severe).
1) Overall Clinical Outcome
The child demonstrated progressive improvement across all symptoms. By the end of the treatment period, complete remission of asthma attacks, resolution of atopic dermatitis, and normalization of bowel habits were observed. No adverse drug reactions were reported, and no allopathic rescue medication was required.
2) Symptom-wise Clinical Assessment Table
| Visit | Respiratory Status | Skin Symptoms | Gastrointestinal Symptoms |
| Baseline | 4 (Severe wheezing, hospitalization required) | 4 (Severe itching, active dermatitis) | 4 (Severe constipation, abdominal pain) |
| 1st Follow-up | 3 | 2 | 3 |
| 2nd Follow-up | 2 | 1 | 1 |
| Final Follow-up | 0 (No asthma attacks) | 0 (Skin clear) | 0 (Normal bowel habits) |
3) Graphical Representation of Clinical Improvement
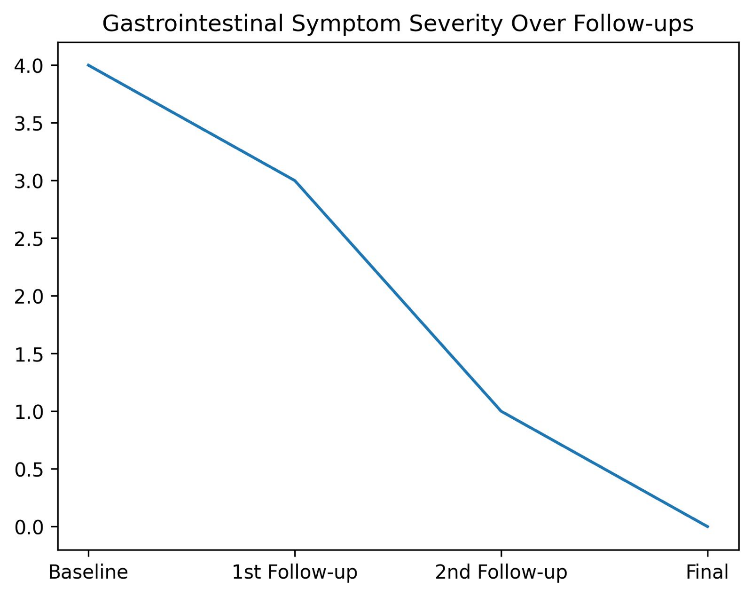
Figure 1 – It illustrates the progressive reduction in gastrointestinal symptom severity. At baseline, the child exhibited severe symptoms (score 4), including constipation, abdominal pain, and regurgitation. During the first follow-up, symptom severity reduced to score 3, followed by further decline to score 1 at the second follow-up. Complete resolution of gastrointestinal complaints was observed at the final visit with a severity score of 0.
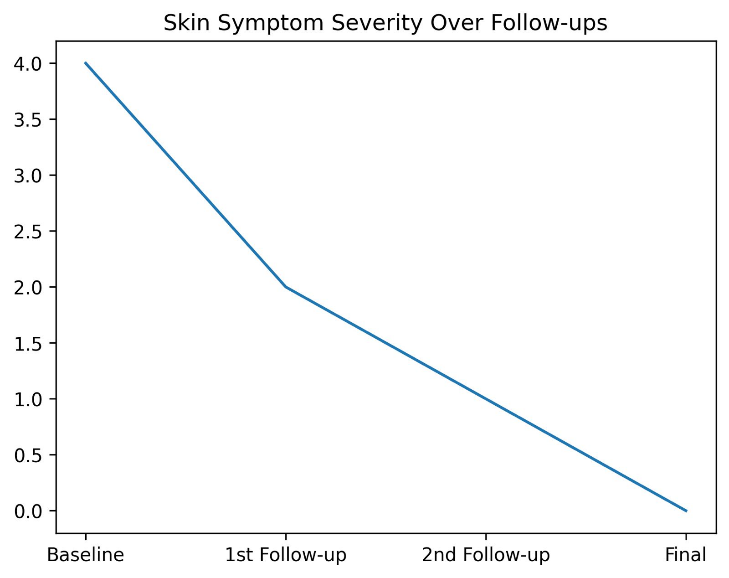
Figure 2 – It represents the improvement in skin manifestations. The baseline score of 4 indicated severe atopic dermatitis with intense itching and dryness. A marked reduction was observed at the first follow-up (score 2), with near complete resolution by the second follow-up (score 1). At the final follow-up, the skin was free from itching and lesions, achieving a score of 0.

Figure 3 – It demonstrates the decline in respiratory symptom severity across successive visits. Initially, the child had severe wheezing and frequent asthmatic attacks with a severity score of 4. The score reduced to 3 at the first follow-up, further decreased to 2 at the second follow-up, and reached 0 at the final follow-up, indicating complete remission from asthma symptoms.
Together, these graphs objectively confirm improvement across gut, skin, and respiratory systems, reflecting successful reversal of cow milk–induced allergic march through Ayurvedic intervention.
4) Key Outcome
- Asthma attacks are completely resolved by the final follow-up.
- Atopic dermatitis lesions healed with the disappearance of itching and dryness. Gastrointestinal symptoms normalized with restoration of regular bowel habits. No recurrence noted during the 5-month observation period.
Discussion
This case demonstrates the successful reversal of cow milk-induced allergic march using Ayurvedic gut-immune modulation treatment. Unlike modern management that focuses on allergen avoidance and symptom suppression, the present treatment corrected the underlying digestive-immune dysfunction, leading to remission of atopic dermatitis and childhood asthma without recurrence.
1) Pathophysiological Understanding
Cow milk protein allergy (CMPA) represents a complex immunological disorder in which exposure to specific milk proteins triggers an exaggerated immune response rather than the development of oral tolerance. In genetically susceptible children, immature gut mucosal barriers allow milk antigens such as α-S1-casein and β-lactoglobulin to penetrate the intestinal epithelium. [1,9]
These antigens are processed by antigen-presenting cells, which preferentially drive naïve T-lymphocytes toward a Th2-dominant phenotype. The resulting cytokine milieu, particularly interleukins-4, -5, and -13, promotes B-cell class switching to IgE, mast-cell sensitization, and eosinophilic inflammation. Repeated exposure perpetuates epithelial barrier damage in both gut and skin, facilitating the progression of allergic march from food allergy to atopic dermatitis and subsequently to bronchial hyper-reactivity and asthma. [10-12]
As per Ayurveda, CMPA is not viewed as a localized immune reaction but as a systemic disorder of digestion and tissue metabolism. Cow milk, described as Guru, Snigdha, Madhura, and Abhishyandi [13], aggravates Kapha Dosha when digestion (Agni) is compromised. Persistent intake under conditions of Agnimandya leads to the formation of Ama, a pathological intermediate that circulates through the body and vitiates multiple Strotas. Involvement of Annavaha and Rasavaha Strotas produces gastrointestinal manifestations such as regurgitation, abdominal pain, and constipation, while affliction of Twak Strotas manifests clinically as Vicharchika in the form of chronic eczema, itching, and dryness.
With continued exposure to the incompatible food (Virudha Aahara), Kapha becomes chronically aggravated and obstructs the physiological movement of Prana Vayu within Pranavaha Strotas. This obstruction (Strotorodha) disturbs the normal respiratory dynamics and gradually evolves into Swasa Roga, explaining the progression from food allergy to childhood asthma observed in this patient. The associated dryness, fluctuating severity, and episodic exacerbations are classical signs of secondary Vata vitiation layered upon the primary Kapha pathology.[14]
Thus, CMPA with allergic march reflects a failure of digestive fire, systemic accumulation of Ama (toxin), progressive channel obstruction, and derangement of Kapha-Vata equilibrium. The disease cannot be effectively reversed by simple allergen avoidance alone, because the Agnimandya, Ama, and Strotodushti persist within the deep root. Restoration of immune tolerance, therefore, requires correction at the level of digestion, tissue metabolism, and channel patency, which formed the therapeutic foundation of the present Ayurvedic treatment.
2) Phase-wise Therapeutic Protocol
| Phase | Duration | Therapeutic Objective |
| Phase I- Allergy control and respiratory stabilization | Sept-Oct 2020 | Reduce allergic load, control asthma, initiate Ama-pachana |
| Phase II- Consolidation Phase | Oct-Dec 2020 | Repair epithelial barrier, suppress inflammatory cascade |
| Phase III- Gut Repair and Immunomodulation | Jan-Mar 2021 | Restore gut integrity, prevent recurrence, and induce immune tolerance |
3) Pharmacological Action of Formulations Used
| Formulation | Key herbs | Pharmacological Action | Ayurvedic Karma | Clinical importance |
| Total Care 3X Ras | Satyanashi, Dronpushpi, Sirisha, Bhoomiamla, Vasa, Dugdhdika, Yavakshara, Yashtimadhu | Antihistaminic, bronchodilator, mast-cell stabilizing, anti-inflammatory | Kapha-Vata Shamana, Kasa-Shwasa Hara | Controlled asthma, reduced allergic hyper-reactivity |
| Respiratory Care X Drops | Vasa, Yashtimadhu, Surasa, Jivanti, Kantkari, Ela, Haridra, Bhoomi Amalaki, Bruhati, Agaru | Bronchodilation, mucolytic, immunomodulatory | Pranavaha Strotas Shodhana | Prevented recurrent wheezing |
| Respiro Detox Formula | Giloy Satva, Tankan Bhasma, Saftik Bhasma, Godanti Bhasma, Abhrak Bhasma | Anti-inflammatory, airway clearance | Kapha-Vilayana, Shwasa Hara | Stabilized chronic asthma |
| Haridra Khandam | Haridra | Antihistaminic, antioxidant | Raktashodhaka, Kaphaghna | Cleared eczema |
| Laxmi Vilas Ras | Classical formulation | Antipyretic, bronchodilator | Kasa-Shwasa Hara | Reduced asthma frequency |
| Aahar Amrutham Bindu | Choti Dudhi, Shrifal, Bhoomiamla, Punarnava | Gut barrier repair, immunoregulation | Deepana, Ama-Pachana | Reversed food intolerance |
| Aahar Amrutham Ras | Choti Dudhi, Shrifal, Bhoomiamla, Punarnava | Mucosal healing, immune tolerance | Rasayana, Agni- Deepana | Prevented relapse |
| E-5 Cell Repair Oil | Karanj, Sirisha, Darvi, Aragwadha, Coconut oil | Anti-inflammatory, wound healing | Twak-Prasadana | Healed atopic lesions |
| IAFA Skin Fresh Bar | Sweta Kutaj, Neelini, Kumari, Lodhra, Nimba, Chakramarda | Antimicrobial, anti-itch | Kandughna | Restored skin barrier |
This case study is the best example of an allergic march. Cow milk allergy initiated immune dysregulation, which progressed into atopic dermatitis and asthma. Modern medicine manages CMPA by food avoidance only, but Ayurveda corrects the pathology at the digestive-immune level by eliminating Ama, restoring Agni, pacifying Kapha, and normalizing Pranavaha Srotas. Five months of structured therapy achieved remission without steroids or inhalers.
Conclusion
This case study revealed that cow milk-induced allergic march is not merely a problem of food exposure but a systemic disorder originating from impaired digestion and immune dysregulation. The child had progressed from food allergy to atopic dermatitis and finally to childhood asthma despite receiving modern symptomatic care. Ayurvedic management based on correction of Ahar Asatmya, restoration of Agni, elimination of Ama, and normalization of Kapha-Vata imbalance resulted in complete clinical remission within five months.
The patient achieved sustained relief from gastrointestinal symptoms, resolution of chronic eczema, and complete freedom from recurrent asthma attacks without the need for corticosteroids, bronchodilators, or other allopathic rescue medication. No adverse effects were observed during treatment, and no recurrence was noted during follow-up.

This case provides clinical evidence that Ayurvedic gut-immune modulation can effectively reverse the allergic march when applied in a structured, phase-wise manner. It supports the role of Ayurveda as a safe and root-oriented therapeutic approach in pediatric cow milk protein allergy with multisystem involvement and highlights the need for larger clinical studies to validate these observations.
References
- Hao L, Wang S, Ji W. Cow’s milk protein allergy: A comprehensive review of epidemiology, pathogenesis, clinical manifestations, diagnostics, and management strategies. Asia Pac J Clin Nutr. 2025 Jun; 34 (3): 298- 307. doi: 10. 6133/ apjcn. 202506- 34 (3). 0004. PMID: 4041- 9390; PMCID: PMC- 12126303.
- Al-Beltagi M, Saeed NK, Bediwy AS, Elbeltagi R. Cow’s milk-induced gastrointestinal disorders: From infancy to adulthood. World J Clin Pediatr. 2022 Nov 9; 11 (6): 437- 454. doi: 10. 5409/ wjcp. v11. i6. 437. PMID: 3643- 9902; PMCID: PMC- 9685681.
- He, M., Hu, J., Deng, J., Chen, X., Liu, C., Olatunji, O. J., Suttikhana, I., & Ashaolu, T. J. (2025). Cow milk allergy: Its clinical aspects, mechanisms, and innovative mitigation strategies beyond enzymatic hydrolysis. Journal of Functional Foods, 130, 106933. https:// doi. org/ 10. 1016/ j. jff. 2025. 106933
- Giannetti, A., Toschi Vespasiani, G., Ricci, G., Miniaci, A., Di Palmo, E., & Pession, A. (2021). Cow’s Milk Protein Allergy as a Model of Food Allergies. Nutrients, 13 (5), 1525. https:// doi. org/ 10. 3390/ nu- 13051525
- Bantz SK, Zhu Z, Zheng T. The Atopic March: Progression from Atopic Dermatitis to Allergic Rhinitis and Asthma. J Clin Cell Immunol. 2014 Apr; 5 (2): 202. doi: 10. 4172/ 2155- 9899.1000202. PMID: 2541- 9479; PMCID: PMC- 4240310.
- Al-Beltagi M, Saeed NK, Bediwy AS, Bediwy HA, Elbeltagi R. Cow milk protein allergy mimics in infancy. World J Clin Pediatr. 2025 Sep 9; 14 (3): 103788. doi: 10. 5409/ wjcp. v14. i3. 103788. PMID: 4088- 1085; PMCID: PMC- 12305122.
- Valenta R, Hochwallner H, Linhart B, Pahr S. Food allergies: the basics. Gastroenterology. 2015 May; 148 (6): 1120- 31. e4. doi: 10. 1053/ j. gastro. 2015. 02. 006. Epub 2015 Feb 11. PMID: 2568- 0669; PMCID: PMC- 4414527.
- Vandenplas Y, De Greef E, Devreker T. Treatment of Cow’s Milk Protein Allergy. Pediatr Gastroenterol Hepatol Nutr. 2014 Mar; 17 (1): 1- 5. doi: 10. 5223/ pghn. 2014. 17. 1. 1. Epub 2014 Mar 31. PMID: 2474- 9081; PMCID: PMC- 3990777.
- Dupont D, Mandalari G, Molle D, Jardin J, Léonil J, Faulks RM, Wickham MS, Mills EN, Mackie AR. Comparative resistance of food proteins to adult and infant in vitro digestion models. Mol Nutr Food Res. 2010 Jun; 54 (6): 767- 80. doi: 10. 1002/ mnfr. 2009- 00142. PMID: 1993- 7605.
- Hill DA, Spergel JM. The atopic march: Critical evidence and clinical relevance. Ann Allergy Asthma Immunol. 2018 Feb; 120 (2): 131- 137. doi: 10. 1016/ j. anai. 2017. 10. 037. Erratum in: Ann Allergy Asthma Immunol. 2018 Apr; 120 (4): 451. doi: 10. 1016/ j. anai. 2018. 02. 033. PMID: 2941- 3336; PMCID: PMC- 5806141.
- Dhar S, Jagadeesan S. Atopic March: Dermatologic Perspectives. Indian J Dermatol. 2022 May- Jun; 67 (3): 265- 272. doi: 10. 4103/ ijd. Ijd- 989- 21. PMID: 3638- 6083; PMCID: PMC- 9644798.
- Haddad EB, Cyr SL, Arima K, McDonald RA, Levit NA, Nestle FO. Current and Emerging Strategies to Inhibit Type 2 Inflammation in Atopic Dermatitis. Dermatol Ther (Heidelb). 2022 Jul; 12 (7): 1501-1533. Doi: 10. 1007/ s13555- 022- 00737- 7. Epub 2022 May 21. PMID: 35596901; PMCID: PMC- 9276864.
- Gore MS, Bhatt A, Mishra SK, Dattani K. Rationalized approach towards milk consumption integrating ayurveda principles and recent advances for health promotion [Internet]. Int J Recent Innov Med Clin Res. 2024, 6 (3): 61- 69. Available from: https:// doi. Org/ 10. 18231/ j. ijrimcr. 2024. 052
- Munblit D, Perkin MR, Palmer DJ, Allen KJ, Boyle RJ. Assessment of Evidence About Common Infant Symptoms and Cow’s Milk Allergy. JAMA Pediatr. 2020; 174 (6): 599- 608. doi: 10. 1001/ jama- pediatrics. 2020. 0153.





